Correcting Severe Bottoming Out
Posted On: November 08, 2021 Author: The Office of Dr. Stuart Linder Posted In: Breast Augmentation, Breast Reconstruction, Plastic Surgery
2 Minute Read:
Repaired by Internal Capsulorrhaphy of the Inframammary Fold
This patient presented with severe scar tissue contracture of the entire collapse of the upper pole of her right breast, causing lowering of the implant with the implant approximately 1.25 inches lower on the right than the left. Not only are her implants too large for her body, the technical error by a previous surgeon caused inferior displacement of the implant due to inadequate release of the superior pectoralis major muscle. The pressure has caused constant inferior creep of the implant down over the last three years.
This technique requires breast implant revision surgery.

This photograph shows that the 397 low profile style 15 gels will be replaced with 350 cc high profile saline implants narrower and smaller. The superior upper portion capsulectomy was performed, rendering complete muscle release up to the clavicle was maintained in the right breast. At this time, you can see the photograph showing the muscle attached down to the intercostal space causing the complete collapse of the upper pole.
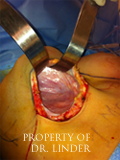
Dr. Linder lifts the capsule along the inframammary fold, which is then released from the inframammary fold of approximately 2.2 cm or one inch.

The capsule is now being sutured up using strong sutures in order to recreate a sling-like effect bringing the implant up and reducing the bottoming out.

The entire capsule has been completely sutured upward and reattached using capsulorrhaphy.

The wound has been closed with large sutures reapproximating the edges. Postoperatively, she now has a double fixation of the inframammary fold with a capsulorrhaphy sling, tighter skin (from the skin excision), and a well positioned nipple-areolar complex.
To schedule your consultation with Dr. Linder or learn more about breast revision surgery, call our office at 310-275-4513 or fill out our online contact form today.