Severe Bottoming Out
Posted On: November 21, 2018 Author: The Office of Dr. Stuart Linder Posted In: Breast Revision, Breast topics, Home
Case Study #1
Reconstruction Inferior Capsulorraphy for Severe Bottoming Out
 Patients present to my practice in Beverly Hills for severe deformities, including malposition, technical areas of breast implant placement, and in this case severe bottoming out, complete collapse of upper pole of pocket causing inferior displacement of the implant and a bottoming out appearance. This is a case example in which the patient will undergo both repair of the bottoming out with an inferior internal capsulorraphy sling as well as a left inframammary tightening procedure of a breast lift nature. Intraoperative photograph shows complete collapse of the upper pole of the pocket with the muscle completely scarred down to just above the level of the 12 o’clock position of the nipple areolar complex. The implant has been pressurized down inferiorly and is approximately 1.5 inches too low. Inferior capsule has been released and a small portion has been excised and has been sutured in place acting as a sling. Skin was then removed and this double tightening procedure has brought the implant level back up to the normal position of the left side. This is a classic example in which a thick capsule can be used as a sling in a capsulorraphy form to treat a patient with severe bottoming out.
Patients present to my practice in Beverly Hills for severe deformities, including malposition, technical areas of breast implant placement, and in this case severe bottoming out, complete collapse of upper pole of pocket causing inferior displacement of the implant and a bottoming out appearance. This is a case example in which the patient will undergo both repair of the bottoming out with an inferior internal capsulorraphy sling as well as a left inframammary tightening procedure of a breast lift nature. Intraoperative photograph shows complete collapse of the upper pole of the pocket with the muscle completely scarred down to just above the level of the 12 o’clock position of the nipple areolar complex. The implant has been pressurized down inferiorly and is approximately 1.5 inches too low. Inferior capsule has been released and a small portion has been excised and has been sutured in place acting as a sling. Skin was then removed and this double tightening procedure has brought the implant level back up to the normal position of the left side. This is a classic example in which a thick capsule can be used as a sling in a capsulorraphy form to treat a patient with severe bottoming out.
Case Study #2
Style 45 Silicone Implants
The below patient presents with severe bottoming out where the implants have fallen significantly and the height distance from the bottom of the areola to the inframammary fold is greater than 13 cm. The patient is a model and declines to have scars throughout her breasts other than the periareolar incision which she previously had.
 Using a style 45, high profile, cohesive silicone Allergen gel implant, we were able to reposition the nipple areolar complex without actually moving the areola by releasing the capsule along the infraclavicular, parasternal and lateral anterior axillary line, replacing the moderate silicone gel implants with a new style 45 cohesive gel implant. This patient has achieved both increased fullness to the upper pole of her breast as well as the nipple areolar complex is now centralized more into the middle of her breast. With certain cases such as this, correction of severe bottoming out can be performed without the use of mastopexies or internal capsulorrhaphies by simply replacing the low or moderate profile saline or silicone implants with the new style 45 cohesive Allergen gel implants.
Using a style 45, high profile, cohesive silicone Allergen gel implant, we were able to reposition the nipple areolar complex without actually moving the areola by releasing the capsule along the infraclavicular, parasternal and lateral anterior axillary line, replacing the moderate silicone gel implants with a new style 45 cohesive gel implant. This patient has achieved both increased fullness to the upper pole of her breast as well as the nipple areolar complex is now centralized more into the middle of her breast. With certain cases such as this, correction of severe bottoming out can be performed without the use of mastopexies or internal capsulorrhaphies by simply replacing the low or moderate profile saline or silicone implants with the new style 45 cohesive Allergen gel implants.
Case Study #3
Full Breast Lift for Breast Revision
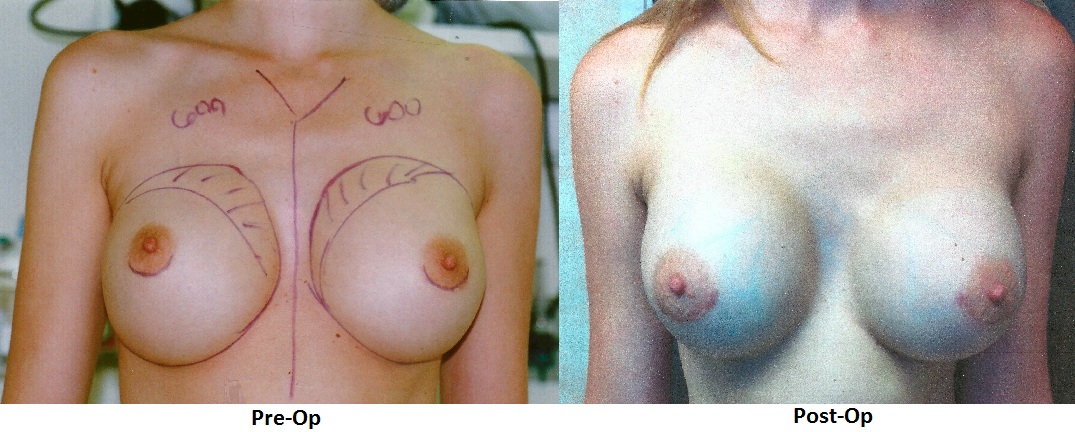
A 41-year-old female body builder came into my Beverly Hills office looking to enhance and correct her breasts from a previous augmentation by another surgeon. During the examination, as you can see by the photo, she has a severe bottoming out. Bottoming out is when the implants has fallen from the bottom of the areola and the inframammary fold. After listening to the her concerns and expectations, we agreed to a surgery date.
During the breast revision surgery, I removed the old 700 cc saline implants and replaced them with 460 cc implants overfilled to 550 Mentor high profile saline. To correct the bottoming out, I performed a sling to bring up the capsule and also a full mastopexy or breast lift to remove the excess skin and tighten the surrounding tissue to reshape and support the new implants.
The patient is only one day post-op, but you can see that the breast are lifted and symmetric.

To schedule your consultation with Dr. Linder or learn more about breast revision surgery, call our office at 310-275-4513 or fill out our online contact form today.