PANNICULECTOMY, THE FINAL STEP AFTER MASSIVE WEIGHT LOSS, WHAT TO EXPECT
Posted On: September 09, 2025 Author: The Office of Dr. Stuart Linder Posted In: Panniculectomy
Everywhere you look today, there’s growing attention on weight loss and body transformation. With medications like Semaglutide—known by brand names such as Ozempic and Wegovy—more people are achieving significant weight loss without surgery. While this is a major step forward for many, it has also led to a noticeable rise in patients seeking panniculectomy and other post-weight-loss body contouring procedures. As plastic surgeons, we’re seeing firsthand how rapid weight reduction, whether surgical or medical, often brings a new challenge: addressing the excess, hanging abdominal skin left behind.
Panniculectomy And A Tummy Tuck: What Is The Difference?
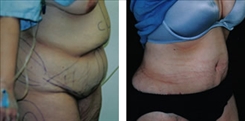
Panniculectomy should be differentiated from an abdominoplasty, also known as a tummy tuck. A panniculectomy is usually associated with incisions of the abdominal pannus, compared to reconstructive abdominoplasty with the muscles of the abdominal wall (rectus sheath plicated). Panniculectomies have commonly been performed with other operations, including gastric bypass surgery (Foley procedure), hysterectomies, and herniorrhaphies, if necessary. Patients who require a panniculectomy, excision of the abdominal pannus or apron, easily show functional signs of the massive abdominal excess skin and fat, which can include hygienic rashes along the suprapubic area that may extend from the inguinal area and the groin creases, up to the hips. The massive amount of weight may also cause functional back pain from the lower and mid-back region, which will be greatly improved by removing this enormous abdominal pannus.
Abdominoplasties normally differ from a panniculectomy in that not only is skin and fat removed, but application of the midline rectus abdominal wall muscles is normally performed. Patients undergoing abdominoplasty usually do not have the same symptoms and functional problems associated with this massive pannus. Literature describes abdominoplasty and panniculectomy as two different procedures. Once again, the panniculectomy is usually only associated with the direct excision of the skin and fat, while abdominoplasty allows for reconstruction of the abdominal wall. A grading system has been developed, associated with a scale of 1 to 5 with the higher grades relating to patients with heavier weight. A correlation has been found that the higher grades have more postoperative problems. The higher grades may also be associated with increased dehiscence of the wound (opening of the wound) with increased rash along the incision site with infection and breakdown of skin. Similar incisions are performed with abdominoplasty and panniculectomy along the lower pubic area extending to the hips; however, often in a panniculectomy a midline incision will be made below the breast bone, extending all the way to the muscle and up to the belly button in order to maintain good blood supply to the thick flap of tissue in order to maintain blood supply of the lower flap to prevent loss of skin which could occur with inadequate blood supply.


Belt Lipectomy
Abdominal panniculectomies should be differentiated from a belt lipectomy. A belt lipectomy usually is associated with direct excision of skin and fat circumferentially around the abdomen as well as the back region above the belt line. This is often performed in patients who have had massive weight loss from gastric bypass or bariatric surgery.
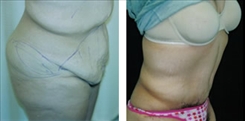
In the video below, Dr. Linder shows a pre-op marking of a patient before her tummy tuck (panniculectomy) surgery. During the surgery, he will be performing liposuction, as well as removing the excess tissue and tightening the abdominal muscles.
Typically, a dermolipectomy or an abdominal/panniculectomy is the removal of loose skin and fat from the lower abdominal area. Tightening of a muscle can often also be performed which would bring the rectus sheath anterior muscle layer to the midline and help tighten up the middle abdominal region. Hernias should be evaluated, especially if it’s palpable on clinical examination, and should be worked up with an ultrasound and if necessary a CT scan if it’s large. It should be referred to a general surgeon and may require the use of a Marlex mesh graft reconstruction of the abdominal wall. Patients who have undergone gastric bypass surgery, especially with upper midline procedural scars in the past, have shown a significant instance of incisional hernias to the upper midline scar and should be evaluated preoperatively with a general surgeon.
Transcription of the above video:
Today we are marking our young lady for a tummy tuck, also referred to as a panniculectomy. The side, I’ll be liposuctioning the hips. This is all the tissue I’ll be removing. And we’ll be lifting up the lower part called the pubic area, tightening all the muscles, going to make a new little hole for the belly button. So look at all this tissue. It’s awesome. This is a great day for her. And all that’s going to be removed. Cute belly button. Cute hips. Two drains at the end.
So that’s called tummy tuck marking.
Potential Complications
Complications associated with either an abdominoplasty or panniculectomy include bleeding such as a hematoma which may be associated with the opening of a vessel which may require returning to the operating room to control the bleeding. Drainage tubes are typically placed for 7 to 10 days until the amount of fluid through the drains is minimal. Infections may be associated with graft placement with concurrent hernia repair as well as skin infections, which may be related to cellulitis or erythema. These must be immediately attended to, usually requiring IV antibiotics in a hospital setting.
Severe scarring can certainly occur along the incision site, and the patient must realize that the scars are always a trade-off for removal of massive amounts of tissue and there can never be a guarantee of the final outcome of any scars. The scars can include keloids, hypertrophic scarring, widespread scarring, hyper or hypopigmentation or a variety of the above. Skin breakdown though rare can occur if dissection is too great, which causes inadequate blood supply to the flap being pulled down.
Other complications can include fluid collections called seroma in which the fluid is formed within the extra abdominal space that was created. This may require a secondary drain placement once again and antibiotics.
Finally, deep venous thrombosis of the legs, which could lead to pulmonary embolism clots in the lungs, can be deadly and patients should have some mobility immediately after surgery, as well as special pneumatic boots within the operating room during the operation to reduce this incidence.
Panniculectomy Revision
Revisions of these large panniculectomies are not uncommon, especially when patients desire to debulk the upper abdominal area, the hip regions or the flanks. We prefer to wait six months prior to liposuction of the upper abdominal or flank areas after abdominoplasty or panniculectomy surgery to reduce the incidents of skin loss or flap death.
Concomitant surgeries are often performed with large panniculectomies for massive weight loss, which may include breast augmentation to regain fullness with or without mastopexies or breast lift to remove the excess skin of the lower breast regions. Brachioplasties (removal of skin from the arms) and thigh plasties, both medial and lateral, may help to smooth out the thigh area with removal of massive amounts of lax skin from the inner and outer thighs. These surgeries are all associated with significant scarring. Once again, the scarring is unpredictable, and the patient must understand the trade-off of the scars for the removal of this massive amount of skin and fat.
Massive panniculectomies are excellent surgeries for the patients who either had massive weight loss by diet and exercise or by bariatric surgery. Similar to breast reduction, patients have a greatly improved quality of life when massive amounts of heaviness of skin and fat that often weighs upon their backs throughout the day are gone, and rashes are also no longer present, and hygienic infections are significantly reduced, including fungal-type infections. Patients commonly feel much improved both in and out of clothing after the surgery.
To schedule your consultation with Dr. Linder or learn more about panniculectomy surgery, call our office at 310-275-4513 or fill out our online contact form today.